|
||
|
|
|
|
||
|
|
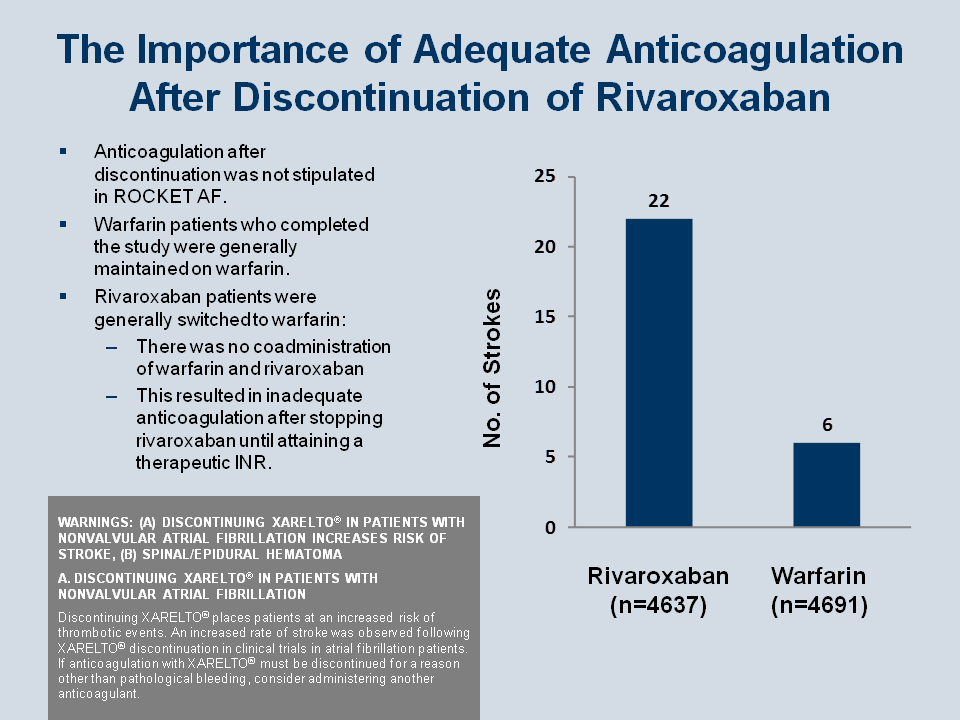
This Figure illustrates an anomaly of the design of ROCKET AF that likely explains some of the difference in results between rivaroxaban and warfarin, but it also illustrates the basis for an important qualification in the use of rivaroxaban.[115] In the design of ROCKET AF, data on events were counted out to 2 days after discontinuation of the assigned drug. However, because of the double-blind design, a patient could not start warfarin in open label if the patient was already on a therapy in ROCKET AF. This means that if a patient on either drug went to early discontinuation and then to open label, it was necessary per protocol to stop the trial drug and before beginning the other anticoagulant. This created a therapeutic imbalance, because if a patient discontinues rivaroxaban and transitioned to open-label warfarin, it takes about 13 days before warfarin will reach serum INR levels in the therapeutic range, whereas up if the patients stop warfarin and start rivaroxaban, the patient achieves therapeutic coverage within a few days. Therefore in the 2 days following discontinuation when events are still be counted, patients discontinuing rivaroxaban and transitioning to open-label warfarin are not receiving adequate therapy, whereas in the reverse situation, rivaroxaban is already providing protection for patients classified as being in the warfarin arm.
This anomaly also provides a possible explanation for the rivaroxaban package insert labeling (dark box in the Figure), which stipulates the necessity for utilizing an alternative anticoagulant regimen if a patient is going to stop rivaroxaban to switch to warfarin.[112]
Reiffel JA. Am J Med 2013; 126: 00-00.
[ Note added in proof: Subsequent to the FDA’s request for the “black box warning” to be added to rivaroxaban, based on the results from ROCKET AF reported in this Figure, a follow-up paper and editorial in JACC suggested that further analysis of ROCKET AF implicated the risks of switching from the NOAC to warfarin, rather than a pharmacologic property of rivaroxaban; from the Editorial:
| | What is clearest from this important subanalysis of the ROCKET AF trial
is that bad things will happen to high-risk AF patients if they are left
untreated with effective anticoagulant therapy for sustained
periods--and that in a population as large as this one, it does not take
much time for those events to begin to accumulate. Although the black
box warning may seem to single out rivaroxaban unfairly in delivering
this message, it at least serves as a reminder that interruptions and
transitions with short-acting anticoagulant drugs must be planned and
managed carefully. | |
Main paper:
Patel MR, Hellkamp AS, Lokhnygina Y, et al. Outcomes of Discontinuing Rivaroxaban Compared With Warfarin in Patients With Nonvalvular Atrial Fibrillation: Analysis From the ROCKET AF Trial (Rivaroxaban Once-Daily, Oral, Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation). J Am Coll Cardiol. 2013;61:651-658.
Editorial:
Reynolds MR. Discontinuation of rivaroxaban: filling in the gaps. J Am Coll Cardiol. 2013;61:659-660.]
[112] Xarelto® (rivaroxaban) film-coated oral tablets [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2011. Revised: November 2012.
[115] ROCKET AF Study Investigators. Rivaroxaban-once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation: rationale and design of the ROCKET AF study. Am Heart J. 2010;159:340-347.