Rader - Figure 11 - Efflux capacity correlates with CAD Text
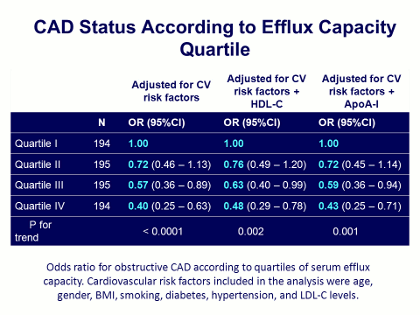
To answer this question of whether the capacity of an individual’s HDL to efflux cholesterol from macrophages (the efflux capacity) correlates with the presence of CAD, we divided the range of efflux capacities measured in this sample into quartiles, from I (with the lowest efflux capacity) to IV (with the highest). We then adjusted these quartiles of efflux capacity for 3 factors: cardiovascular disease (CV) risk factors, CV risk factors plus HDL cholesterol level, and CV risk factors plus ApoA-I levels.
As shown in this Table, when the 4 efflux capacity quartiles were adjusted for CV risk factors, the chances (odds ratio) of having CAD in quartile IV (individuals with the highest, ie, healthiest efflux capacity) versus in quartile I (the lowest) was 0.4, p<0.0001. (Put another way, the individuals whose HDL had the highest cholesterol effluxing capacity had a 60% lower probability of having angiographically proven CAD.) When the same efflux capacity quartiles were adjusted for baseline HDL levels, there was again a diminished probability for the presence of CAD, although the odds ratio was now 0.48, p<0.002. (There was, incidentally, an association, or correlation, between HDL cholesterol level and overall efflux capacity, but this was not terribly strong.)
Then in the final column, the same procedure was repeated but this time adjusting for the principal apolipoprotein on HDL particles, apoA-I, and again, increasing efflux capacity was associated with a highly statistically significant decrease in the odds ratio for having angiographically proven CAD.
These data are consistent with the idea that this measurement of HDL function, cholesterol efflux capacity, is actually an independent predictor of risk, even after controlling for HDL or apoA-I levels. In other words, even after adjusting for an individual’s baseline HDL or ApoA-I level, cholesterol efflux capacity was still a predictor of angiographic CAD.
J Clin Lipidol. 2011; 5(6).