Another issue that has to be taken into account when discussing the epidemiologic studies of HDL cholesterol and clinical trial results is how independent the changes in HDL cholesterol are as a predictor of events.
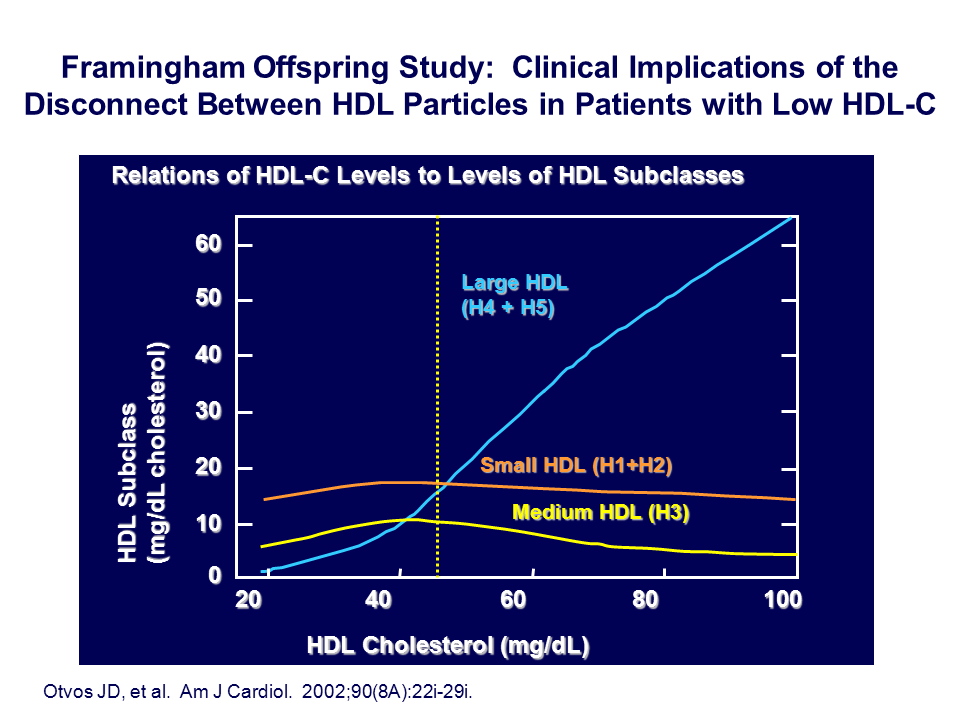
In the Framingham Offspring Study,[41] the relationship between HDL cholesterol, HDL subclasses, and LDL subclasses was explored. Higher serum HDL cholesterol levels are associated with a higher concentration of large, cholesterol-enriched HDL particles and a lower concentration of the small and medium cholesterol-depleted HDL particles (Figure 6). However, because the enzymatic pathways in the transfer proteins that affect HDL also affect LDL, individuals with low serum levels of HDL cholesterol have high concentrations of cholesterol-depleted small LDL particles; conversely, higher concentrations of HDL cholesterol are associated with lower concentrations of large, buoyant LDL particles (Figure 7). So the lower the HDL cholesterol, the higher the concentration of the small, dense LDL particles, and the higher the concentration of the total number of LDL particles.
We know from many prospective studies[42] that LDL particle concentration, which can be quantitated because each LDL particle has a single apolipoprotein B, is a superior predictor of CVD risk than serum LDL cholesterol level. So if there is an inverse relationship between HDL cholesterol and high numbers of LDL particles (or apo-B containing lipoproteins), the question is, whether the risk related to the low levels of HDL cholesterol, or is it related to the excess number of LDL particles?
This is a very important consideration that one has to consider in statistical modeling: what is the extent of statistical adjustment that has to occur in order to relate HDL cholesterol as a biomarker to the endpoint that we are evaluating, be it changes in vascular imaging or be it changes in CVD events?
With the marked prevalence of the metabolic syndrome and diabetes throughout the developed world these days, these issues concerning the LDL/HDL interactions must be addressed, because individuals who are insulin resistant are the ones who have the small, cholesterol-depleted HDL particles and concomitantly the small, dense cholesterol- depleted LDL particles – which is where apoB becomes even more important as a predictor of future CVD events. These issues were recently highlighted in the American Diabetes Association (ADA)/American College of Cardiology (ACC) consensus statement,[43] and the American Association of Clinical Chemistry guidelines.[44]
J Clin Lipidol. 2011; 5(6).[41]Otvos, JD, Cromwell, W, Shalaurova, I, Schaefer, EJ. LDL particles, but not ldl cholesterol, are highly elevated in the metabolic syndrome: results from the Framingham Offspring Study. Circulation 2003; 108 (Suppl IV):740.
[42]Cullen P. Evidence that triglycerides are an independent coronary heart disease risk factor. Am J Cardiol. 2000; 86: 943–949
[43]Brunzell JD, Davidson M, Furberg CD, et al. Lipoprotein management in patients with cardiometabolic risk. Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31(4):811-822.
[44]Contois JH, McConnell JP, Sethi AA, Csako G, Devaraj S, Hoefner DM, Warnick GR ; AACC Lipoportiens and Vascular Diseases Division Working Group on Best Practices. Clin Chem. 2009; 55:407-419