Eikelboom - Evidence from the Randomized Trials - Figure 9
New Oral Anticoagulants
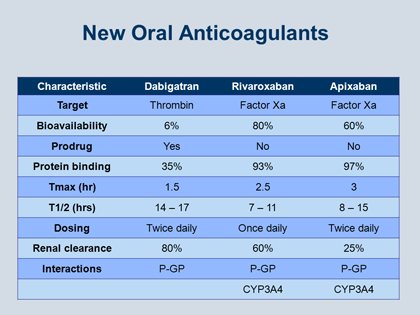
The characteristics of the 3 new NOACs – dabigatran, rivaroxaban, and apixaban – are summarized in Figure 9. The first important distinction between them is that dabigatran targets thrombin, whereas rivaroxaban and apixaban target factor Xa; there are also some important differences in their bioavailability: dabigatran has a low bioavailability, whereas for rivaroxaban and apixaban the bioavailability is a lot higher.
However, while these characteristics – whether a drug targets Xa or IIa, or whether a drug has high or low bioavailability – are interesting, it is really an academic exercise, because for our patients, all that really matters is whether the drug is effective.
Another characteristic that is of academic interest but has no material impact on patient care is whether the prescribed drug is really a prodrug (eg, dabigatran) or the drug works instantly without having to be transformed to its active metabolite (eg, rivaroxaban and apixaban).
Differences in protein binding, on the other hand, are relevant for patient care. For example, in the unusual situation where it is necessary to remove a drug using dialysis, if the drug is highly protein-bound, it is impossible to remove with dialysis. This means that neither rivaroxaban or apixaban are amenable to clearance through dialysis, whereas dabigatran, which is only about 35% protein bound, can be partially removed with dialysis.
For all 3 of these new agents the time to maximum concentration (Tmax) is between 1 and 3 hours. This is important to bear in mind, because it means that the drug will start working as soon as the patient begins taking it, and within a couple of hours the therapeutic effect of the drug will be close to maximal.
The biolobic half-life (T1/2) of all 3 of these drugs is around 12 hours, and this too has implications for patient care. It means that the drug must be administered at least once or twice daily, and if a patient misses 2 or 3 doses, the anticoagulant effects are suddenly rather low. The latter result is important because a patient who is not adherent can rapidly run into trouble. On the flip side, a patient who needs surgery or needs interruption of treatment for bleeding will have a rapid dissipation of the anticoagulant effect.
The last important distinction between the agents concerns renal clearance, and again this is an issue that is relevant for patient care. Dabigatran is almost entirely dependent on renal function for its clearance, whereas rivaroxaban and apixaban are much less dependent on renal function for clearance. For clinicians this means that in patients with markedly impaired renal function, the Xa inhibitors rivaroxaban and apixaban might be preferred over dabigatran.
Drug/Drug Interactions
Unlike with the VKAs, for these NOACs drug/drug interactions are not a major issue. There are only a few drugs that can interfere with the activity of each of these agents, namely drugs that are strong inhibitors or inducers of P-glycoprotein as well as drugs that affect P-glycoprotein, the gut and renal transporter, as well as cytochrome P450 3A4 (CYP3A4).
For dabigatran, the important drugs of concern for interference are ketoconazole, quinidine, and rifampicin. There are some other drugs that are less important but still require attention, such as amiodarone and verapamil. In the case of amiodarone and verapamil, these are not contraindicated in patients taking dabigatran, but physicians should be aware of the potential for an interaction.
Both rivaroxaban and apixaban have similar drug-interaction profiles, for ketoconazole is again one of the drugs that can cause drug/drug interactions. Other drugs that can interfere with the factor Xa inhibitors include some of the macrolide antibiotics and some of the HIV protease inhibitors. There are also less commonly used drugs, such as cyclosporine and tacrolimus, that also require attention for possible drug/drug interference with the factor Xa inhibitors.
In summary, this is a short but an important list of considerations that physicians should bear in mind when prescribing these NOACs for use in patients. Eikelboom J. Am J Med 2013; published on-line at http://education.amjmed.com/00000.